Anxiety disorders are the most common psychiatric conditions in childhood, affecting approximately one in eight children. They are also among the most responsive to treatment when recognized early and addressed with evidence-based interventions. Yet anxiety in children frequently goes unrecognized, dismissed as shyness, behavioral defiance, or a phase that will pass.

Drawing on major child psychiatry textbooks, this article provides clinicians and parents with an evidence-based framework for understanding, recognizing, and responding to childhood anxiety.
How Anxiety Presents in Children
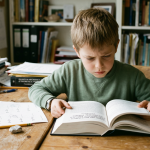
Childhood anxiety does not typically look like adult anxiety. Children rarely say “I feel anxious” or “I am worried about this specific thing.” Instead, they present behaviorally: refusing to go to school, complaining of headaches or stomachaches, becoming clingy and refusing to separate from parents, or having explosive emotional reactions to seemingly minor triggers. These behaviors are often misinterpreted as defiance, manipulation, or physical illness rather than recognized as manifestations of anxiety.
The most common presentations include separation anxiety disorder, where the child becomes intensely distressed when separated from attachment figures; generalized anxiety disorder, characterized by pervasive worry about school, health, safety, and other domains; and social anxiety disorder, where fear of negative evaluation from peers leads to avoidance. Each presentation has distinct features, but all share the core characteristic of excessive, developmentally inappropriate fear that impairs functioning.
Key clinical fact: One in eight children meet criteria for an anxiety disorder. Among those affected, fewer than half receive treatment. Cognitive-behavioral therapy is first-line, with strong evidence for both individual and group formats. For moderate to severe presentations, combining CBT with SSRI medication produces better outcomes than either treatment alone.
What Works: Evidence-Based Treatment
Cognitive-behavioral therapy is the first-line psychosocial treatment for childhood anxiety. CBT for children typically involves psychoeducation about anxiety, cognitive restructuring, graded exposure to feared situations, and skills training. Parent involvement in treatment consistently improves outcomes, particularly for younger children. The therapist teaches parents how to respond to anxious behavior in ways that support the child’s progress rather than inadvertently reinforcing it.
When anxiety is moderate to severe or when CBT alone is insufficient, SSRI medication — particularly fluoxetine and sertraline — has strong supporting evidence. The combination of CBT and medication produces better outcomes than either alone for moderate to severe presentations.
What Parents Can Do
| Instead of | Try this |
|---|---|
| Reassuring the child that nothing bad will happen | Acknowledge the fear: “I can see this feels really scary.” Validate the emotion before addressing the cognition. |
| Allowing the child to avoid feared situations | Gently support facing the fear. Avoidance strengthens anxiety. Each avoided situation makes the next one harder. |
| Solving the problem for the child | Collaborate: “What could we try together that might help?” Building agency is itself therapeutic. |
Conclusion
Childhood anxiety is common, recognizable, and treatable. The gap between prevalence and treatment is not a gap in effective interventions — it is a gap in recognition, in access, and in the willingness of adults to take children’s fears seriously. Every child whose anxiety is identified early and treated appropriately has a trajectory altered — not by magic, but by the consistent application of interventions that the evidence has already validated.