
Adolescents are easy to misread. They may speak with adult vocabulary, argue with adult confidence, and reject help with adult irritation. But adolescence is not adulthood with worse manners. It is a developmental period with its own biology, social pressures, identity work, privacy needs, and risks.
Williams and Hill’s chapter "Teenagers" makes one point especially clear: thirteen and nineteen are not the same. The teenage years contain enormous variation. A good assessment does not treat all teenagers as one species, and it does not treat them as broken adults.
The central adolescent contradiction
Teenagers want autonomy and protection at the same time. They may want to set their own rules, but still need adults to hold boundaries. They may reject emotional language, but still need someone to notice distress. They may say little in front of parents, then become thoughtful when seen alone.
That contradiction is not hypocrisy. It is development.
For clinicians and parents, this means that a teenager’s refusal, sarcasm, silence, or apparent indifference should not automatically be interpreted as lack of need. It may be embarrassment, distrust, loyalty conflict, fear of consequences, or a test of whether the adult can remain steady.
Why seeing the teenager alone matters
A joint family meeting can show patterns, but it can also hide information. Some teenagers will not discuss peers, substances, sexuality, self-harm, bullying, shame, or family conflict in front of parents. Others will perform toughness in front of clinicians. Some will protect parents from painful truths.
A private conversation is not a rejection of parents. It is often a way to make the assessment more accurate. Confidentiality should be explained clearly, including its limits when safety is at risk.
What changes clinically in adolescence
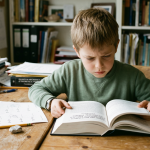
Adolescence is when many important difficulties become more visible: mood disorders, anxiety, self-harm, eating disorders, substance use, trauma responses, psychosis risk, identity distress, and conduct problems. But the symptom alone is rarely enough. The assessment must ask how the problem interacts with school, peers, sleep, family, online life, and future expectations.
A teenager who is not attending school may be depressed, bullied, exhausted, autistic, sleep-deprived, using substances, frightened of failure, or making a rational protest against an environment that feels impossible. Sometimes more than one explanation is true.
Adults should avoid fake coolness
Teenagers usually detect forced relevance quickly. Adults do not need to know every platform, song, meme, or slang term. They do need to be honest, curious, and able to tolerate embarrassment without becoming defensive.
Better than pretending to know is saying: "I may not know the details, but I want to understand what it means to you."
A practical assessment checklist
| Area | What to ask |
|---|---|
| Autonomy | Where does the teen want more control, and where do they still want help? |
| Safety | Any self-harm, suicidal thoughts, exploitation, violence, or risky substance use? |
| Privacy | What cannot be said in front of parents or school? |
| Sleep | Bedtime, phone use, morning functioning, weekend shift. |
| Peers | Belonging, rejection, bullying, online pressure. |
| Family | Conflict, protection, expectations, cultural rules. |
| School | Learning, attendance, shame, workload, teacher relationships. |
For digital context, see Peer Pressure in the Digital Age and Screen Time and Children’s Social Skills.
Source notes
Book source: Williams J, Hill P. The Art of Child and Adolescent Psychiatry. Cambridge University Press. Volume 1, Assessment, section A: The Child. Chapter A3, "Teenagers," pp. 22-27.
External sources used for context: NIMH on the teen brain, AAP media use guidance, Steinberg’s developmental account of adolescent risk taking (Developmental Review), and CDC youth mental health resources.
Verification note: This article is original prose, based on the book chapter and public evidence sources.